Workbook (PDF)
A workbook containing elements of psychoeducation and skills-development.
This comprehensive psychoeducational guide helps clients understand paranoid and suspicious thoughts, their impact, the factors that can contribute to the experience, and evidence-based treatment approaches, including cognitive behavioral therapy.
A workbook containing elements of psychoeducation and skills-development.
Paranoid and suspicious thoughts exist on a spectrum, ranging from everyday mistrust and vigilance to severe persecutory beliefs that significantly impact wellbeing, relationships, and daily functioning. This guide is designed to be an accessible introduction for helping clients understand paranoia through a cognitive-behavioral lens.
The guide explores the experience of paranoia, the psychological mechanisms that can contribute to and maintain it, and the options for treatment. Through clear explanations and real-world examples, clients are supported in making sense of their experiences without judgment.
Paranoia can be distressing, isolating, and difficult for clients to discuss openly. Many people experiencing suspicious thoughts feel misunderstood, ashamed, or uncertain about whether their concerns are justified. This resource provides a compassionate and evidence-based way to normalize these experiences while helping clients develop a deeper understanding of the factors that influence them.
The guide is particularly valuable for psychoeducation and early intervention. It helps clients understand how threat beliefs, attention biases, worry, sleep difficulties, and coping behaviors can contribute to persistent suspicious thinking.
Clients experiencing paranoia, persecutory beliefs, or psychotic symptoms.
Individuals whose trauma-related threat perceptions contribute to suspicious thinking.
Clients whose feelings of vulnerability and negative self-beliefs contribute to paranoia.
Individuals whose threat monitoring and worry increase suspicious interpretations.
People whose loneliness and disconnection contribute to increased threat perceptions
Individuals whose sleep disruption contributes to unusual experiences and suspicious thinking.
Clients whose paranoia may be exacerbated by alcohol or drug use.
Introduce the guide early in therapy to normalize experiences and build understanding.
Discuss the case examples to help clients recognize similar processes in their own experiences.
Map threat beliefs, unusual experiences, attentional biases, and coping strategies.
Support clients understanding about confirmation bias, threat monitoring, and jumping-to-conclusions reasoning.
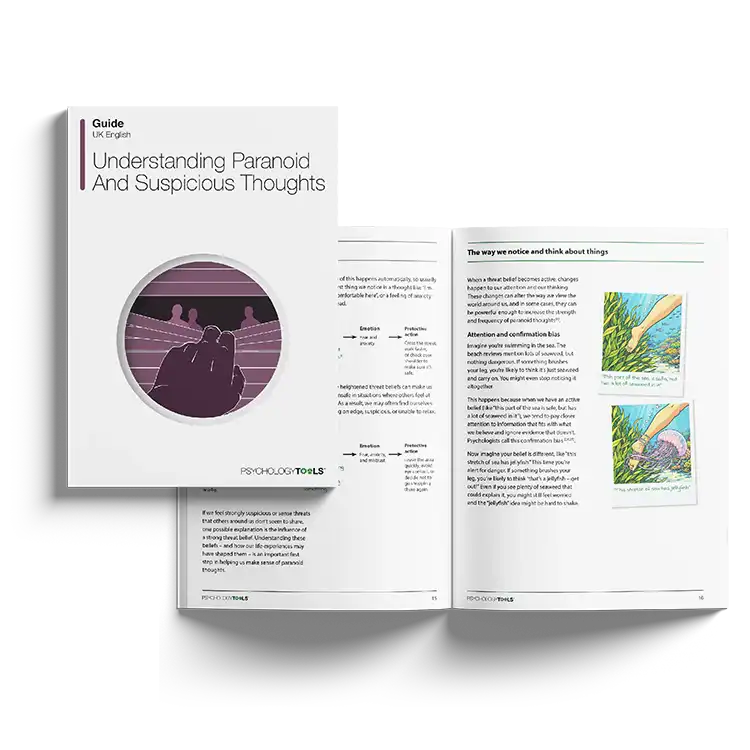
This guide is grounded in contemporary cognitive models of paranoia, which propose that suspicious thoughts emerge when individuals perceive themselves as vulnerable, other people as threatening, or the world as dangerous. These threat beliefs are often shaped by adverse experiences such as trauma, bullying, abuse, discrimination, social exclusion, or chronic stress.
The guide describes how activated 'threat beliefs' influence attention and interpretation. Individuals become more vigilant for signs of danger, more likely to notice information that confirms their fears, and less likely to attend to evidence suggesting safety. These processes are reinforced by mechanisms such as confirmation bias and a tendency to make rapid judgments under perceived threat.
The guide also highlights the important role of worry, sleep disturbance, unusual experiences, and avoidance behaviors. Worry narrows attention toward potential dangers, poor sleep increases emotional vulnerability and unusual experiences, and safety behaviors can prevent clients from discovering that feared outcomes may not occur. Together, these factors can create self-reinforcing cycles that maintain paranoia over time.
For therapists, the guide offers an excellent foundation for psychoeducation. It can be used to introduce cognitive-behavioral concepts, encourgae the development of individualized maintenance cycles, and prepare clients for interventions such as cognitive restructuring, behavioral experiments, sleep interventions, anxiety management, and relapse prevention planning.
This guide supports improved outcomes by helping clients understand their experiences through a coherent psychological framework. Increased understanding often reduces confusion, shame, and self-criticism while enhancing engagement in treatment.
Clients gain insight into the relationship between threat beliefs, cognitive biases, emotional distress, and coping behaviors. This understanding creates opportunities for meaningful cognitive and behavioral change.
For clinicians, the resource provides a structured psychoeducational foundation that can strengthen case formulation, improve treatment engagement, and support the implementation of evidence-based CBT interventions for paranoia and related difficulties.
Working...