Professional version
Offers theory, guidance, and prompts for mental health professionals. Downloads are in Fillable PDF format where appropriate.
A licensed copy of Fairburn and colleagues (2003) cognitive behavioral model of anorexia nervosa (AN) which describes a framework to address key components of AN.

Offers theory, guidance, and prompts for mental health professionals. Downloads are in Fillable PDF format where appropriate.
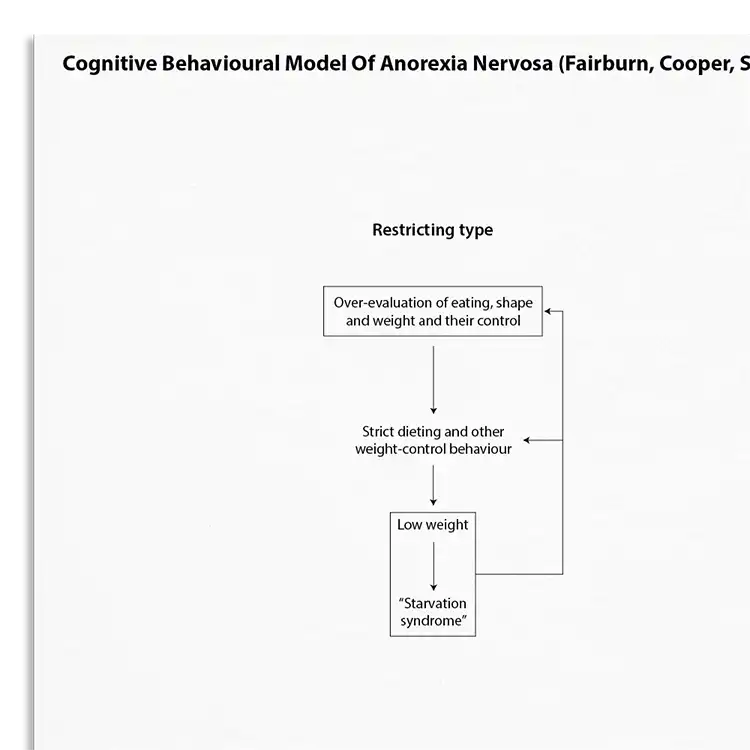
Anorexia nervosa is an eating disorder characterized by restriction of energy intake and intense fear of gaining weight. For women, the lifetime prevalence of developing anorexia is between 1.2 and 2.2% (Smink et al, 2012). This is a cognitive behavioral model of anorexia nervosa, and forms part of the transdiagnostic model of eating disorders.
Understanding the key underpinnings of anorexia nervosa (AN) is important for effective intervention. This resource helps clinicians to:
Including restrictive and binge-purging subtypes.
Understand more about the cognitive behavioral model of anorexia nervosa.
Use the model as a template to organize your case formulations.
Use your knowledge of the model to explain maintenance processes to clients.
Engage clients in discussions about their beliefs and behaviors.
Customize interventions based on individual maintenance mechanisms.
Use in supervision to discuss case conceptualizations and treatment plans.
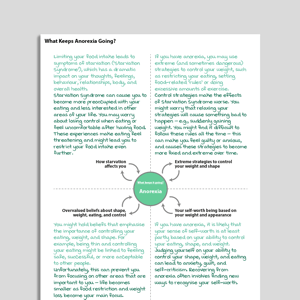
Fairburn, Cooper and Shafran (2003) suggest that over-evaluation of eating, shape and weight, and their control is central to the maintenance of anorexia nervosa. They propose that this cognitive process drives dieting and weight control behavior which results in ‘starvation syndrome’ and further cognitive changes. Their model of anorexia nervosa presented here describes the maintenance of both a ‘restricting type’ and a ‘binge-eating / purging type’.
In their extended transdiagnostic theory of eating disorders (of which the present maintaining processes form a part) the authors identify a number of additional maintenance mechanisms which operate in some cases of anorexia nervosa. These include clinical perfectionism, core low self-esteem (persistent and pervasive negative self-beliefs that are viewed as part of the individual’s self-identity), mood intolerance (difficulty coping with strong mood states), and interpersonal difficulties. One interesting characteristic of the full transdiagnostic model is that “The patient’s specific eating disorder diagnosis is not of relevance to the treatment. Rather, its content is dictated by the particular psychological features present and the processes that appear to be maintaining them”.

Working...