Professional version
Offers theory, guidance, and prompts for mental health professionals. Downloads are in Fillable PDF format where appropriate.
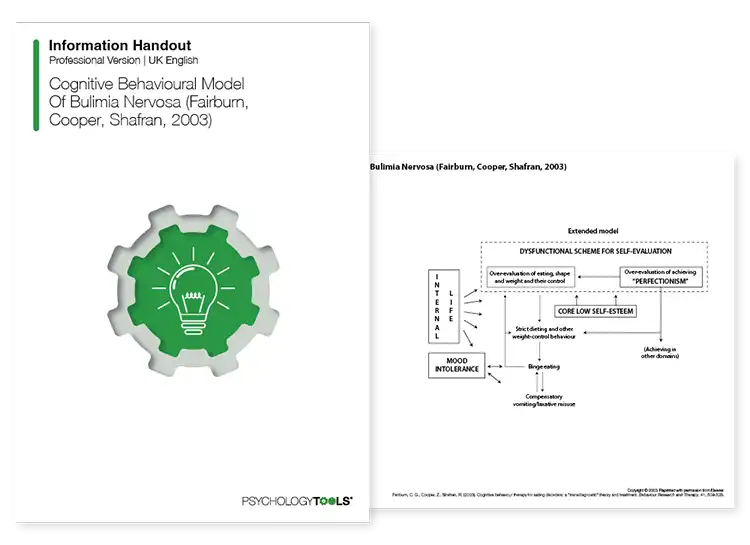
A licensed copy of Fairburn and colleagues (2003) cognitive behavioral model of bulimia nervosa (BN) which describes a framework to address key components of BN.
Offers theory, guidance, and prompts for mental health professionals. Downloads are in Fillable PDF format where appropriate.
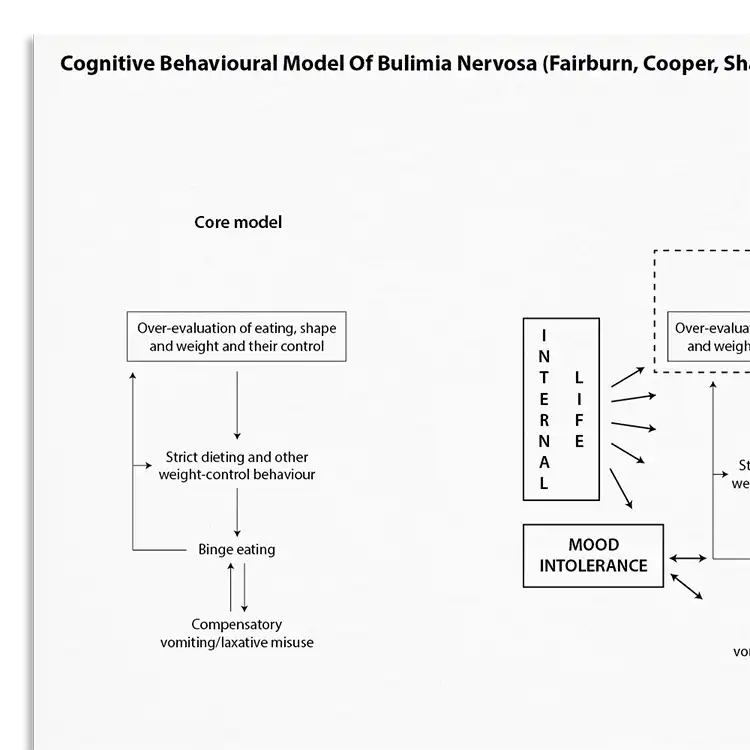
Bulimia nervosa is characterized by episodes of binge eating accompanied by compensatory behaviors like self-induced vomiting or excessive exercise to prevent weight gain. Fairburn, Cooper, and Shafran developed a cognitive-behavioral model illustrating how these behaviors stem from an over-evaluation of eating, shape, and weight control as primary measures of self-worth (Fairburn, Cooper, & Shafran, 2003).
Understanding the key underpinnings of bulimia nervosa (BN) is important for effective intervention. This resource helps clinicians to:
Designed to help individuals affected by bulimia nervosa (BN).
Understand more about the cognitive behavioral model of bulimia nervosa (BN).
Use the model as a template to organize your case formulations.
Use your knowledge of the model to explain maintenance processes to clients.
Engage clients in discussions about their beliefs and behaviors.
Customize interventions based on individual maintenance mechanisms.
Use in supervision to discuss case conceptualizations and treatment plans.
Fairburn, Marcus and Wilson (1993) proposed that a dysfunctional system for evaluating self-worth is primary to the maintenance of bulimia nervosa. Instead of evaluating one’s self-worth based on a broad range of criteria they argue that people with bulimia judge themselves largely, or even exclusively, in terms of their eating habits, shape, or weight (and often all three) and their ability to control them. The ‘problems’ of bulimia nervosa, such as weight-control behavior and preoccupation with weight, are seen as resulting from this primary mechanism.
In the extended 2003 theory a number of additional maintenance mechanisms were added to the model. It was proposed that these only operate in some patients, and include clinical perfectionism, core low self-esteem (persistent and pervasive negative self-beliefs that are viewed as part of the individual’s self-identity), mood intolerance (difficulty coping with strong mood states), and interpersonal difficulties.
Fairburn, Cooper and Shafran (2003) proposed a transdiagnostic model of eating disorder, of which this model of bulimia forms a part. One interesting characteristic of the treatment is that The patient’s specific eating disorder diagnosis is not of relevance to the treatment. Rather, its content is dictated by the particular psychological features present and the processes that appear to be maintaining them.

Working...