Professional version
Offers theory, guidance, and prompts for mental health professionals. Downloads are in Fillable PDF format where appropriate.
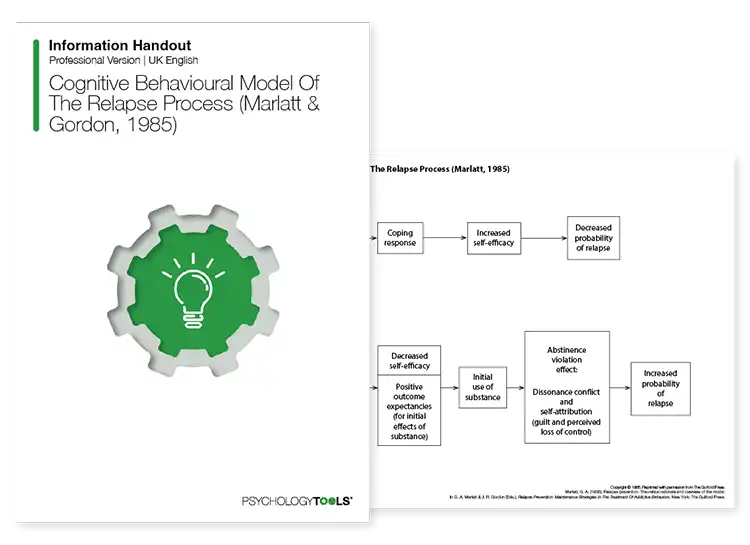
A licensed copy of Marlatt and Gordon's (1985) model of relapse, which describes key aspects of the relapse process.
Offers theory, guidance, and prompts for mental health professionals. Downloads are in Fillable PDF format where appropriate.
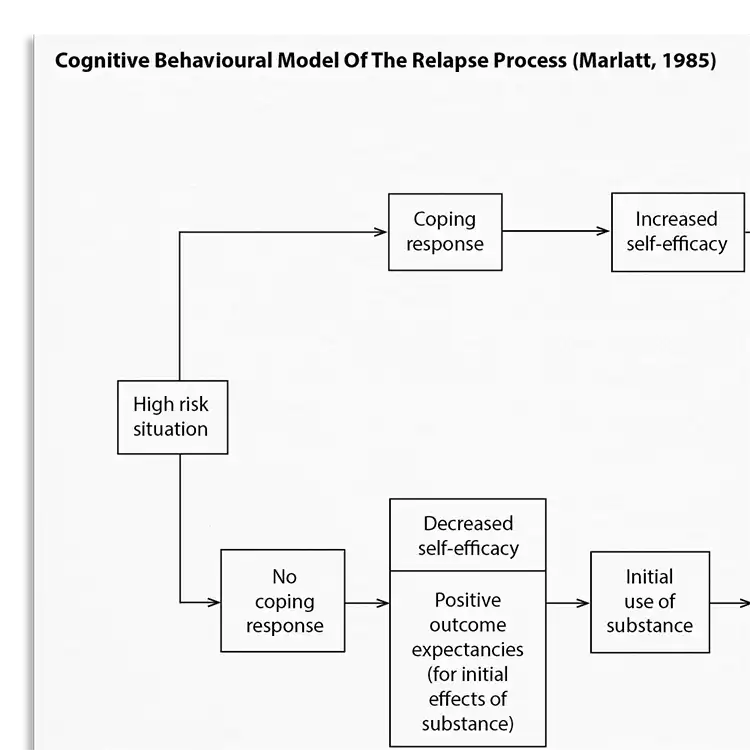
Marlatt & Gordon’s cognitive behavioral model of relapse (1985) conceptualizes relapse as a “transitional process, a series of events that unfold over time” (Larimer et al., 1999). The full model provides a detailed taxonomy of the factors which can lead to relapse episodes.
Understanding what contributes to lapses and relapses is important for effective intervention. This resource helps clinicians:
Identifying and managing high-risk situations to prevent relapses.
Using relapse prevention to prevent the return of eating disorder symptoms, such as binge-eating.
Understand more about the cognitive behavioral model of relapse.
Use the model as a template to organize your formulation of lapses and relapses.
Use your knowledge of the model to explain how and why relapses occur.
Engage clients in discussions about their experience of relapsing
Use in supervision to discuss treatment plans.
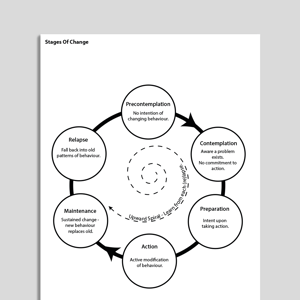
Marlatt and Gordon’s (1985) cognitive behavioral model of relapse conceptualizes relapse as a “transitional process, a series of events that unfold over time” (Larimer et al., 1999). This is in contrast to alternative models which view relapse as an end-point or ‘treatment failure’. Flexibility is a key advantage of such transitional models: they provide guidance and opportunities for intervening at multiple stages in the relapse process in order to prevent or reduce relapse episodes.
Marlatt and Gordon’s full model provides a detailed taxonomy of the factors which can lead to relapse episodes. Larimer et al (1999) describe how these factors fall into two core categories: (1). immediate determinants (such as high-risk situations, or an individual’s coping skills), and (2). covert antecedents (such as an imbalanced lifestyle which leads to urges and cravings).
The cognitive behavioral model of relapse helps clinicians to develop individualized treatment plans for clients at risk of relapse. While the model was designed for working with clients struggling with alcohol problems it has been applied to addictive and impulsive behaviors more broadly (Marlat & Donovan, 2005) including problematic eating behaviors (Mines & Merrill, 1987).

Working...