Professional version
Offers theory, guidance, and prompts for mental health professionals. Downloads are in Fillable PDF format where appropriate.
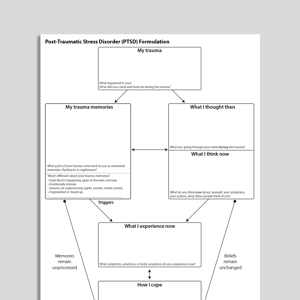
A licensed copy of Ehlers and Clark (2000) cognitive behavioral model of post-traumatic stress disorder (PTSD).
Offers theory, guidance, and prompts for mental health professionals. Downloads are in Fillable PDF format where appropriate.
This professional handout describes the cognitive-behavioral model of PTSD by Ehlers and Clark (2000). The model serves as a comprehensive framework for understanding how PTSD is maintained through problematic memory processes, negative appraisals, and maladaptive coping strategies. It outlines how products of the traumatic event, such as intrusive memories and appraisals of the experiences, result in a heightened experience of current threat, and directs therapists towards effective avenues for intervention.
The Ehlers and Clark model (2000) is a cornerstone for treating PTSD, providing insights into the psychological processes that maintain the disorder. This handout aids clinicians in:
Developing and refining interventions for clients with this diagnosis.
Working with complex trauma, emotional dysregulation, and interpersonal difficulties rooted in prolonged exposure to traumatic experiences.
Early intervention in clients exposed to trauma.
Addressing dissociative symptoms and the impact of trauma on self-experience and reality perception.
Evaluate your client's experience of trauma, their memories, and their cognitive processing during trauma.
Highlight maladaptive appraisals and coping strategies.
Work on evaluating and altering negative appraisals of self, others, and the world.
Help clients re-engage with previously avoided activities and situations.
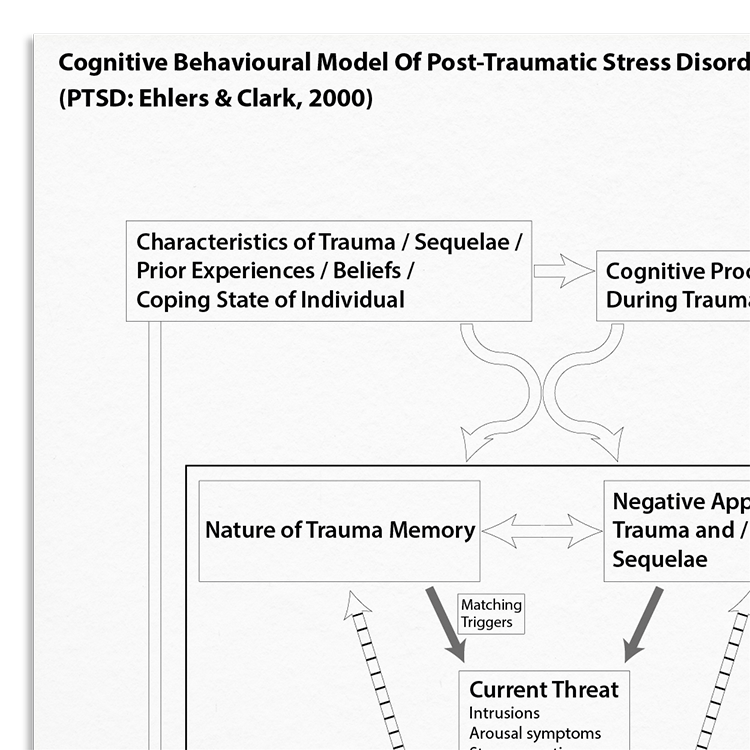
Ehlers and Clark's model (2000) conceptualizes PTSD as a sense of current threat, maintained by memory characteristics, negative appraisals, and ineffective coping behaviors. Trauma memories are experienced as involuntarily vivid with sensory characteristics resulting in charactersitic re-experiencing symptoms. Negative appraisals, both of the trauma and subsequent symptoms, contribute significantly to perceived ongoing danger and emotional distress. Coping strategies, often intended to mitigate threat perceptions, such as avoidance and thought suppression, can hinder recovery by preventing trauma processing and maintaining negative appraisals. Ehlers and Clark's insight is that effective treatment should thus focus on memory elaboration, appraisal modification, and strategic behavior change to break the cycle of perceived threat.

Clinicians benefit from a structured framework for assessing and treating PTSD and related symptoms.
Working...