Guide (PDF)
A psychoeducational guide. Typically containing elements of skills development.
An accessible and informative guide to understanding depersonalization and derealization, written specifically for clients.
A psychoeducational guide. Typically containing elements of skills development.
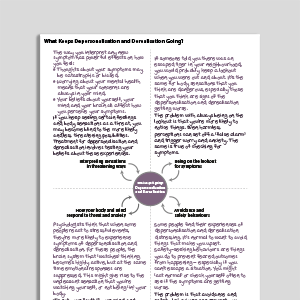
Our ‘Understanding…’ series is a collection of psychoeducation guides for common mental health conditions. Friendly and explanatory, they are comprehensive sources of information for your clients. Concepts are explained in an easily digestible way, with plenty of case examples and accessible diagrams. Understanding Depersonalization And Derealization is designed to help clients who experience depersonalization and derealization to understand more about their condition.
This guide aims to help clients learn more about depersonalization and derealization. It explains what these difficulties are, common symptoms associated with them, and effective ways to address them, such as cognitive behavioral therapy (CBT).
Designed to help clients understand and learn more about DPD.
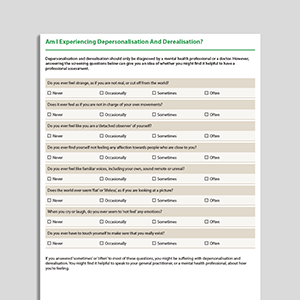
Identify clients who may be experiencing depersonalization disorder (DPD).
Provide the guide to clients who could benefit from it.
Use the content to inform clients about DPD and help normalize their experiences.
Discuss the client’s personal experience with DPD.
Plan treatment with the client or direct them to other sources of help and support.
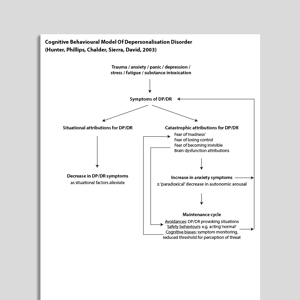
At some point in their lives - often when tired or under physical or psychological stress - many individuals experience brief episodes of feeling detached either from themselves or from the world around them. Feeling detached from oneself is referred to as depersonalization; clients might describe this as feeling as though they are dreaming or observing themselves from a distance, as if through glass. Feeling detached from the external world is known as derealization, where the surroundings may seem unfamiliar, artificial, or unreal.
Brief experiences of depersonalization and derealization are common and generally not a cause for concern. However, when these experiences become frequent, more intense, and begin to interfere with daily functioning, clients may be suffering from depersonalization-derealization disorder. It is estimated that between 1% and 2% of the population experience this disorder, with many individuals enduring symptoms for extended periods before seeking help. Encouragingly, cognitive behavioral therapy (CBT) has been shown to be an effective treatment for depersonalization and derealization.

Working...